These tumours include;
- Giant cell tumor
- Ewing’s tumor
- Adamantinoma
GIANT CELL TUMOR
Presentation
This is a benign tumor, which can have an aggressive process. It may also rarely metastasize to the lungs (<2%). Malignancy rates increase if there is local recurrence. This is more common in young females (20-50 years), and is uncommon in children with open physes.(19% of benign tumors). It usually occurs in the epiphysis or epimetaphysis of the long bones, with 50% occurring about the knee, with the vertebra, radius and sacrum in other cases. Multicentricity occurs in < 1% of patients. Pain is the usual symptom, referable to the involved joint, perhaps with mild swelling. Serum Calcium is usually normal.
Imaging
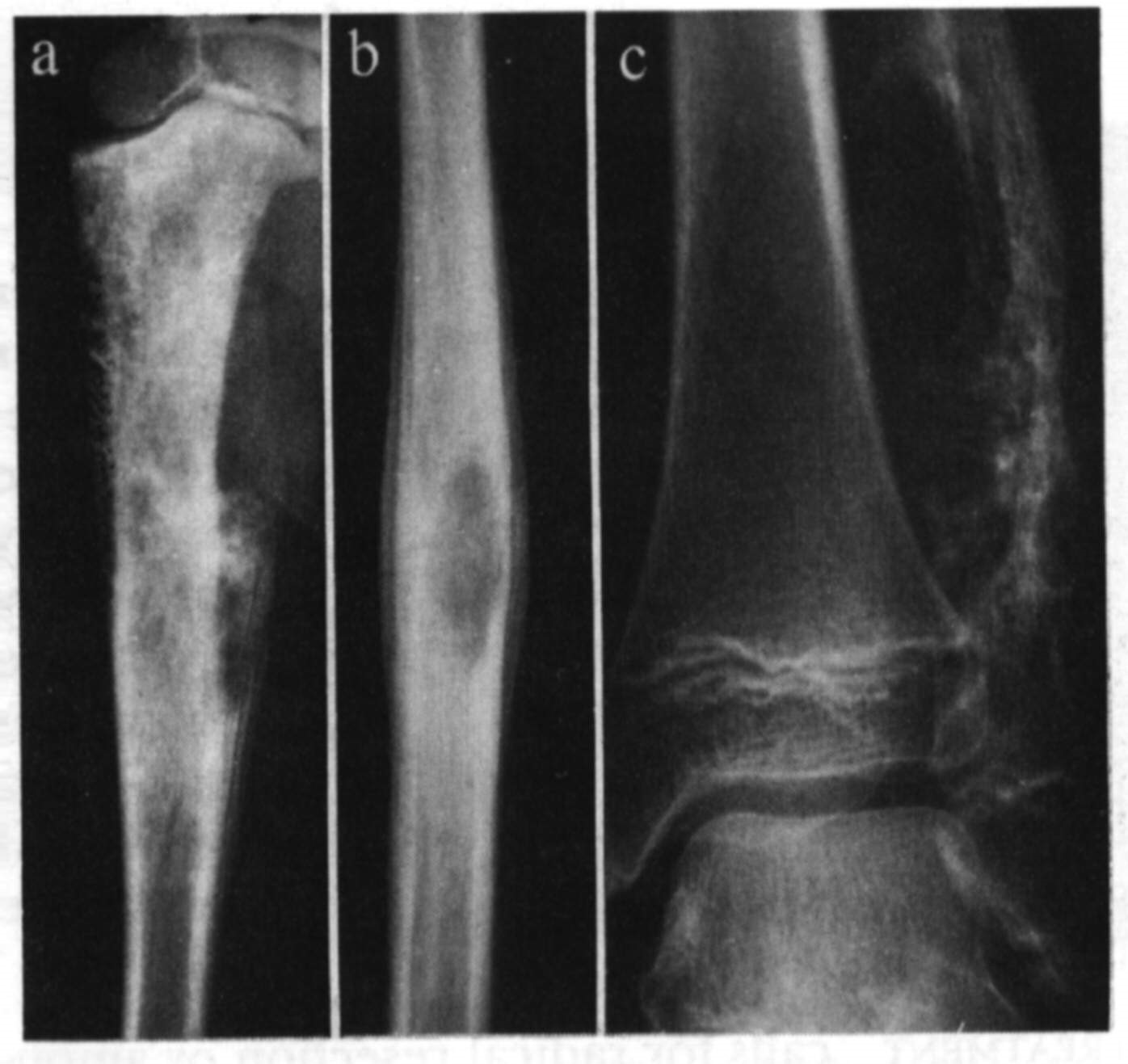
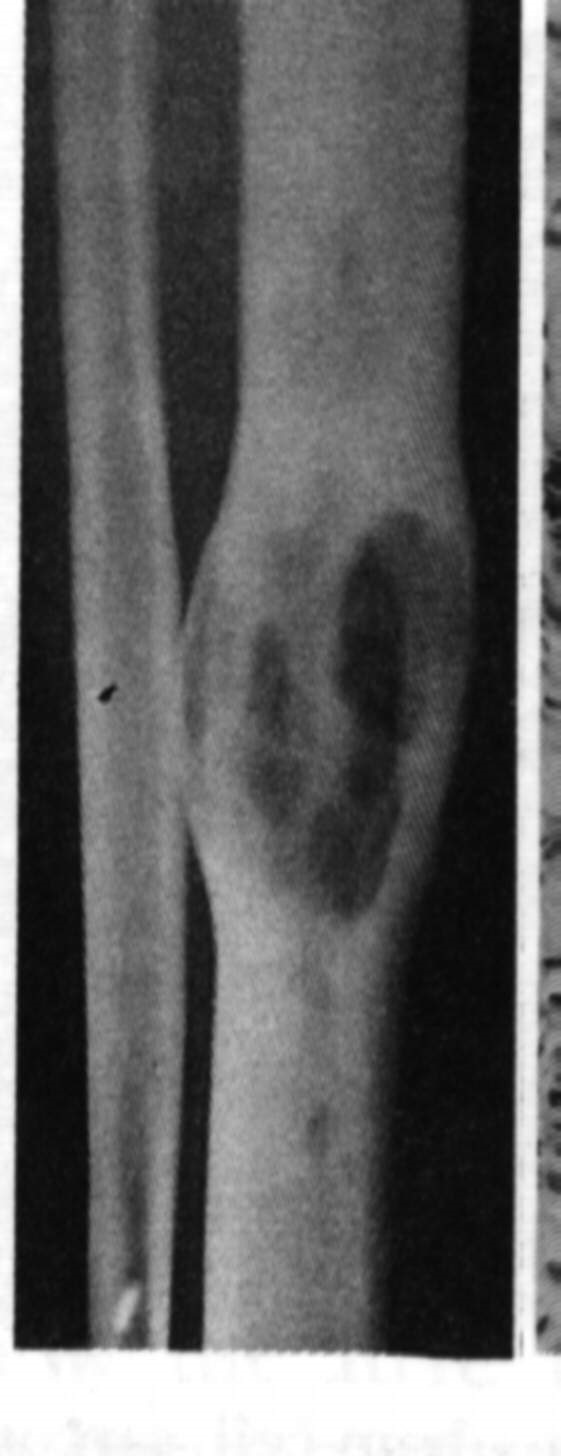
X-ray shows a purely lytic, destructive lesion eccentrically in the end of a long bone, mainly in the epiphysis, often extending up into the subchondral plate. The endosteal margin may be ill defined. The centre often has a soap bubble appearance, and the cortex is thinned and ballooned. In aggressive lesions, there may be soft tissue extension. To determine it’s behavior, CT, bone scanning and MRI scans are used, as well as distant systemic imaging.
Histology
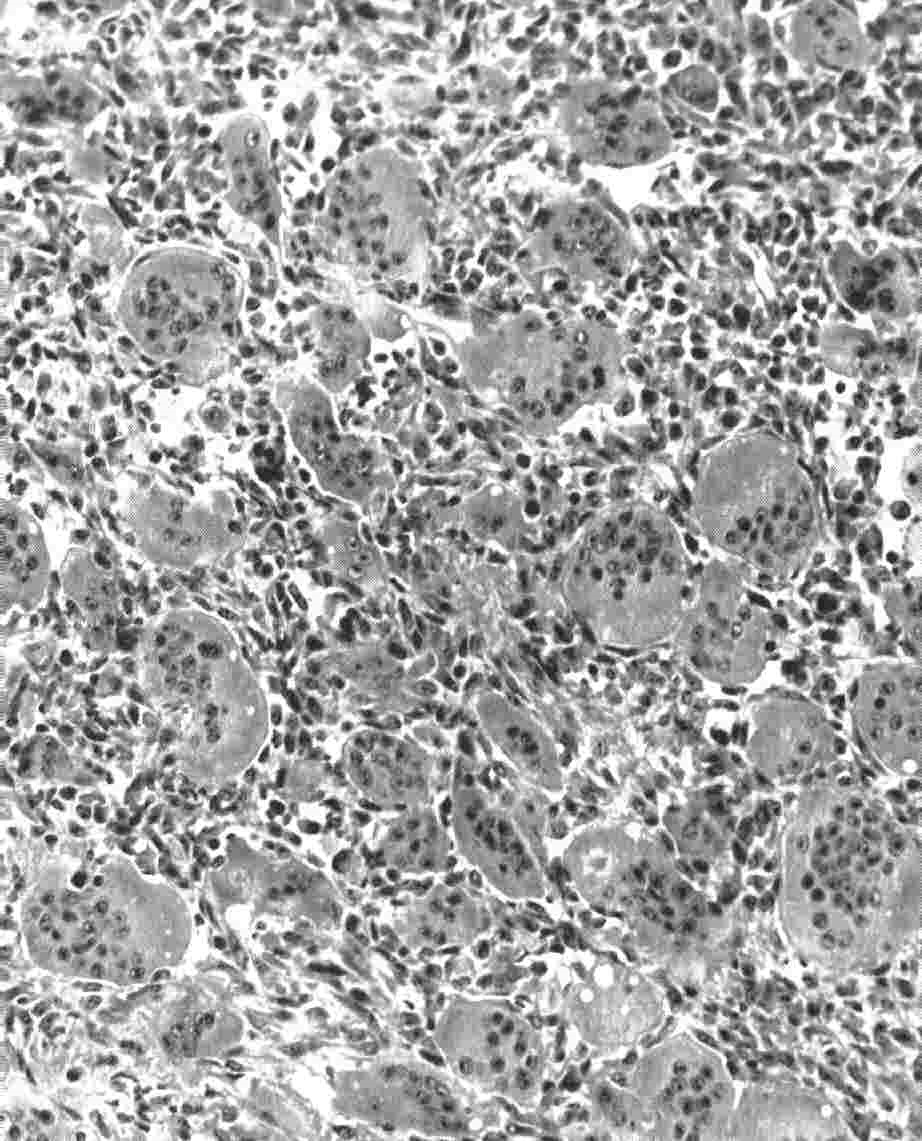
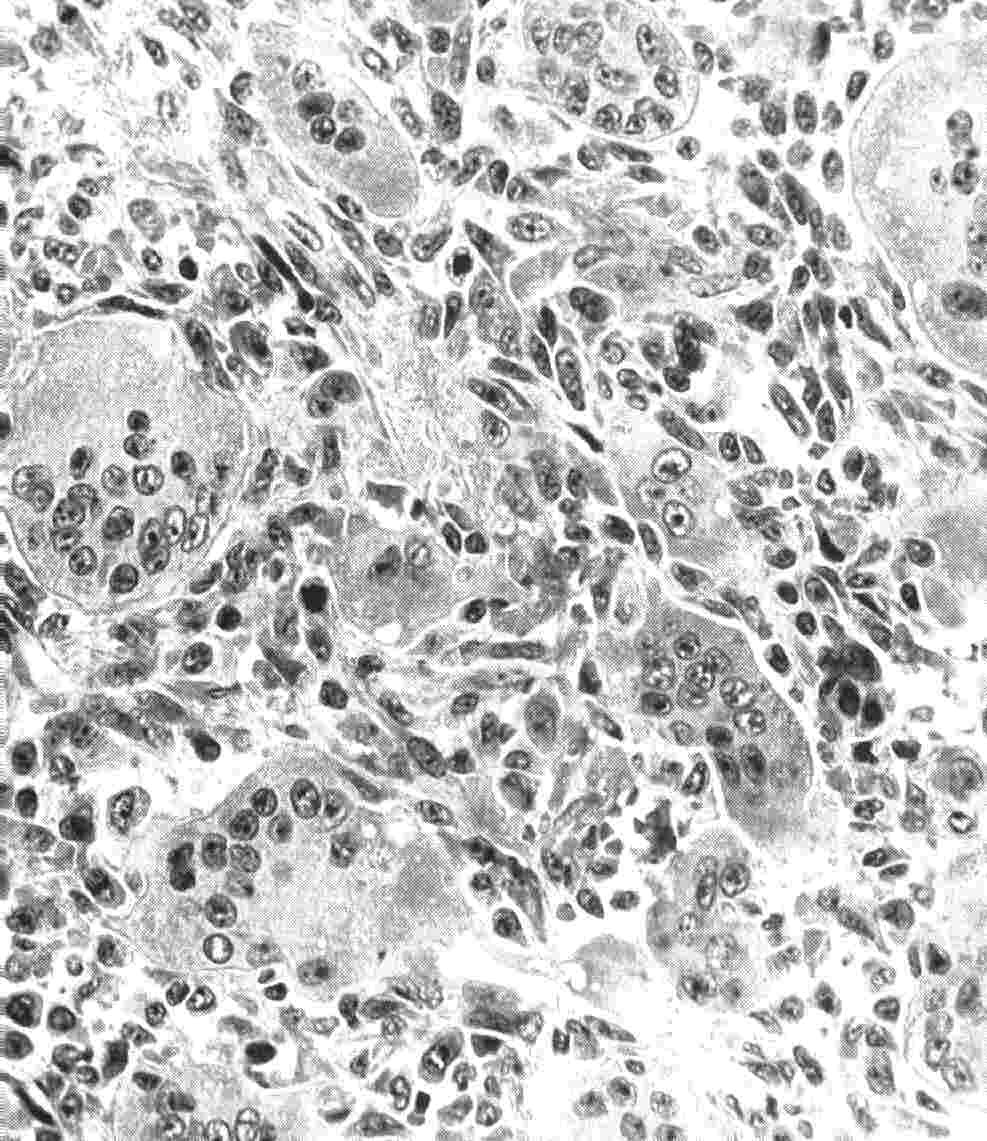
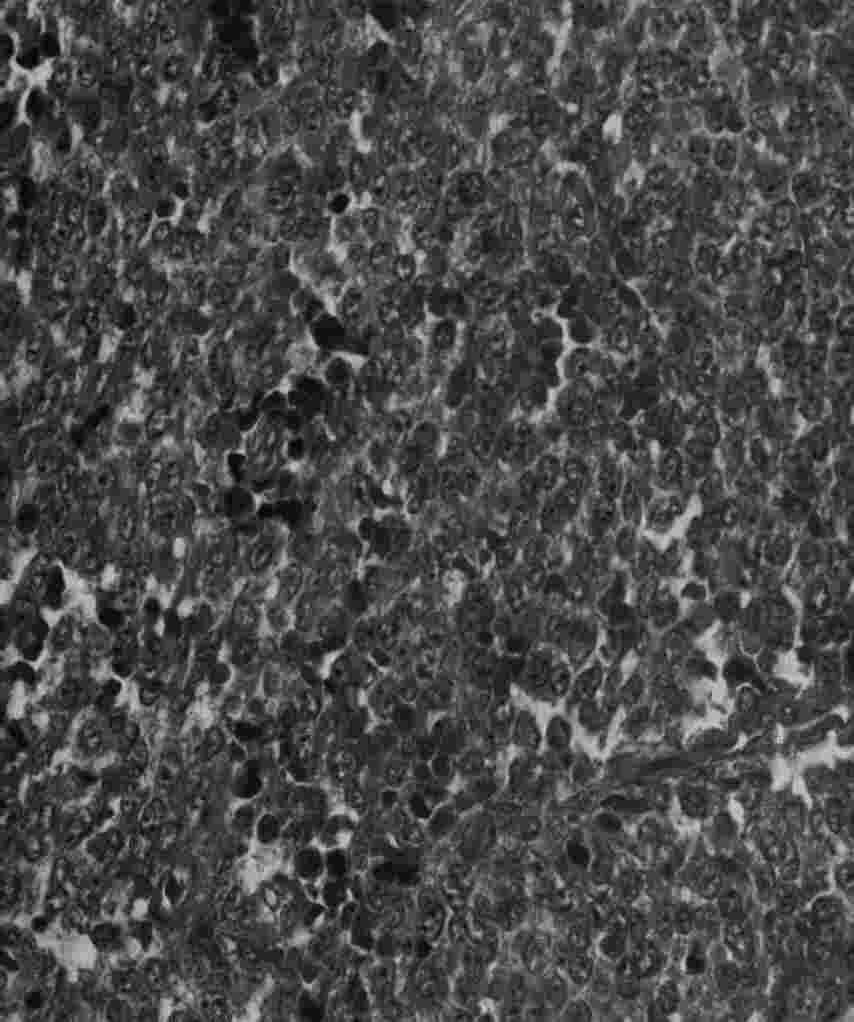
The tumor is reddish in appearance, and comes away in pieces, and may have a poorly defined edge if it’s an aggressive tumour. The basic cell is the giant cell, which has a round/oval shaped nucleus. This multinucleated cell is set in a background of spindle shaped stromal cells, with numerous mitotic figures, and very little intercellular tissue. These giant cells are thought to related to osteoclasts, as they possess all the characteristics of osteoclasts. This contrasts to the giant cells in other lesions, which don’t. This may account for the resorption of bone.
Staging
A stage 1 tumor (Campanacci), is one which causes symptoms, appears latent radiographically, and has a benign histology. A stage 2 tumor, has a more aggressive radiological appearance, with no metastases, and a benign histology. A stage 3 tumor has a very aggressive X-ray, with soft tissue extension, but still a benign histology.
Treatment
This is aimed at removing the lesion, with preservation of the joint. This means extended intralesional curettage though a cortical window, +/- phenol or liquid nitrogen cauterization, with bone graft or bone cement. (80% control). If using cement, the cartilage surface must be cooled with saline, to prevent heat necrosis. Another option is en bloc resection, with allograft, but this does have some problems. Radiation therapy can be considered when surgical excision is not feasible. (e.g. vertebrae).
 |
 |
Sheets of multinucleated giant cells can be seen
 |
 |
EWING’S TUMOR
Presentation
These tumors occur in small children and young adults, 10-20 years. Patient’s present with pain, fever may be present, and there may be local swelling and warmth. Lab tests show an increase in ESR, WCC and anaemia. Characteristically the flat and axial bones are involved. Visceral, lymphatic and meningeal involvement can occur.
Imaging
X-rays show a large destructive lesion that often involves the metaphysis and particularly the diaphysis (unlike osteosarcoma), they may be lytic, or show variable amounts of new bone formation. The periosteum may be lifted off in many layers, giving the uncommon but characteristic onion skinning. There is usually a large soft tissue component,(CT and MRI). A bone scan/PET is necessary to look for other bone involvement.
Histology
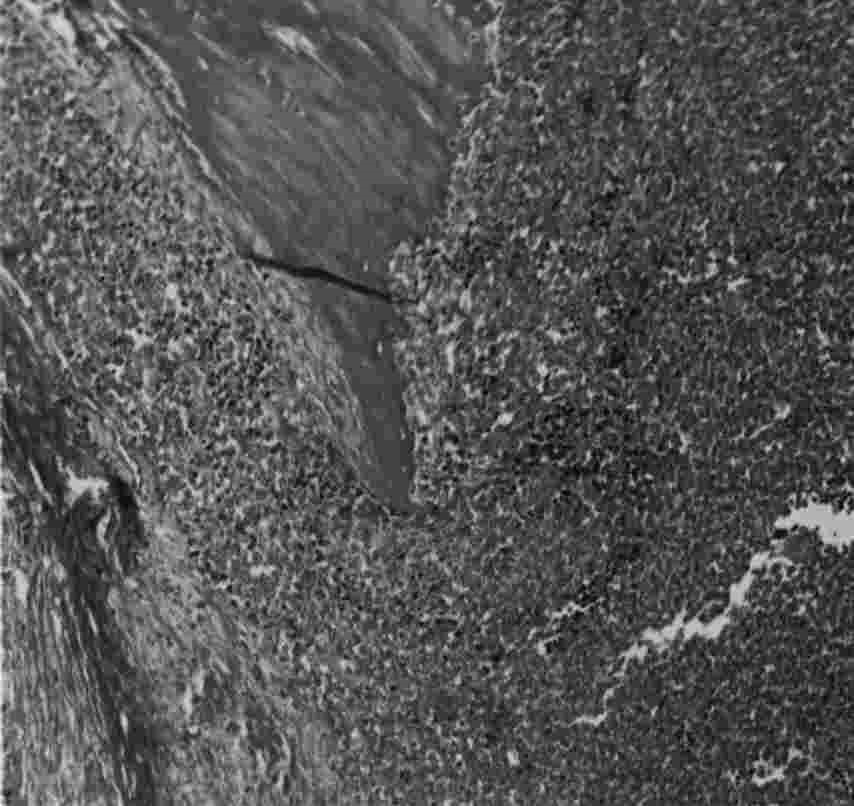
This is a small round blue cell tumour, which is believed to arise from the endothelial cells in the bone marrow (primitive neurectodermal cell). Macroscopically it is lobulated, grey in colour. Microscopically it has sheets of small dark polyhedral cells, with no regular arrangement and no ground substance.
Treatment
This involves a combination of multi agent chemotherapy (e.g.Doxorubicin, cyclophosphamide), surgical resection, +/- irradiation (4500-6000cGy). Long term survival may be as high as 60-70%.
 |
 |
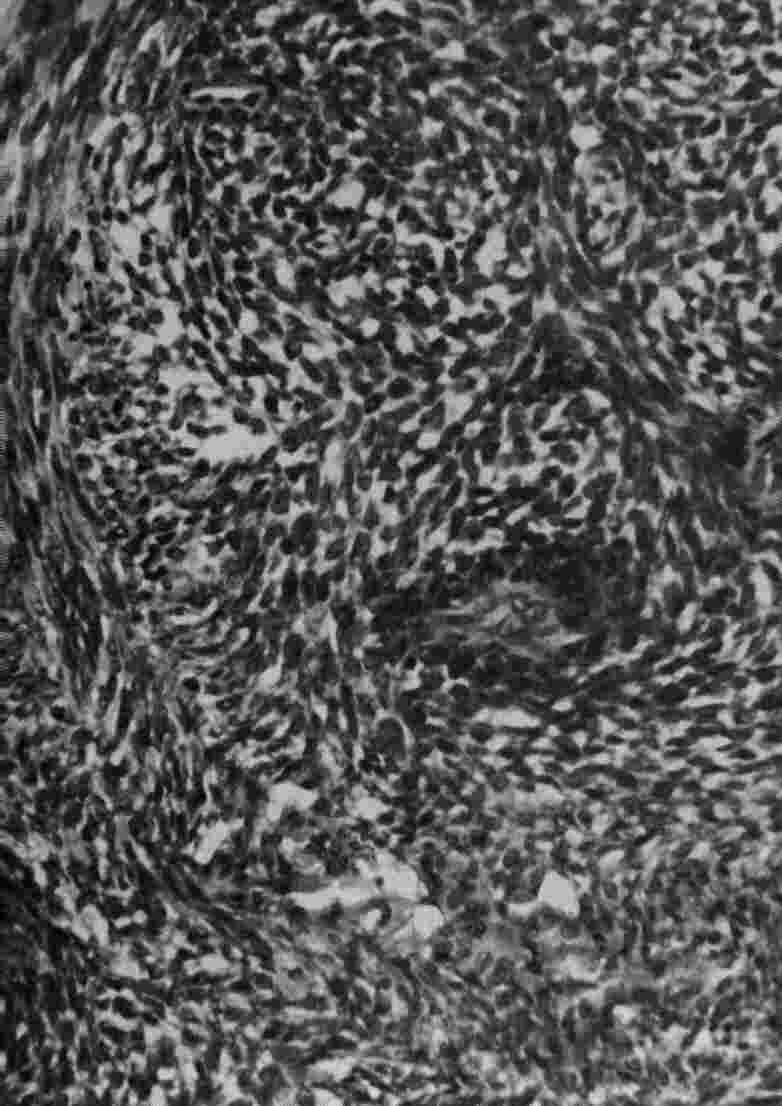
Low power shows bone surrounded by a highly cellular neoplasm, with the high power showing the sheets of round cells.
ADAMANTINOMA
Presentation
This is a rare malignant tumour, and is found often in the tibia, and occasionally in the other long bones. Most patients are young adults who present with long term pain, particularly over the tibia, with mild swelling or local bony deformity. Clinically there is thickening and tenderness along the subcutaneous boarder of the tibia.
Imaging
This shows on X-ray as multiple sharply circumscribed lucent defects of different sizes, with sclerotic bone between these lucency’s.
Histology
The cells in this tumor have an epithelial like quality, and are arranged in a palisading or glandular pattern, surrounded by a fibrous stroma.
Treatment
This involves wide surgical resection, as the lesion may metastasize, usually late after incomplete removal.
 |
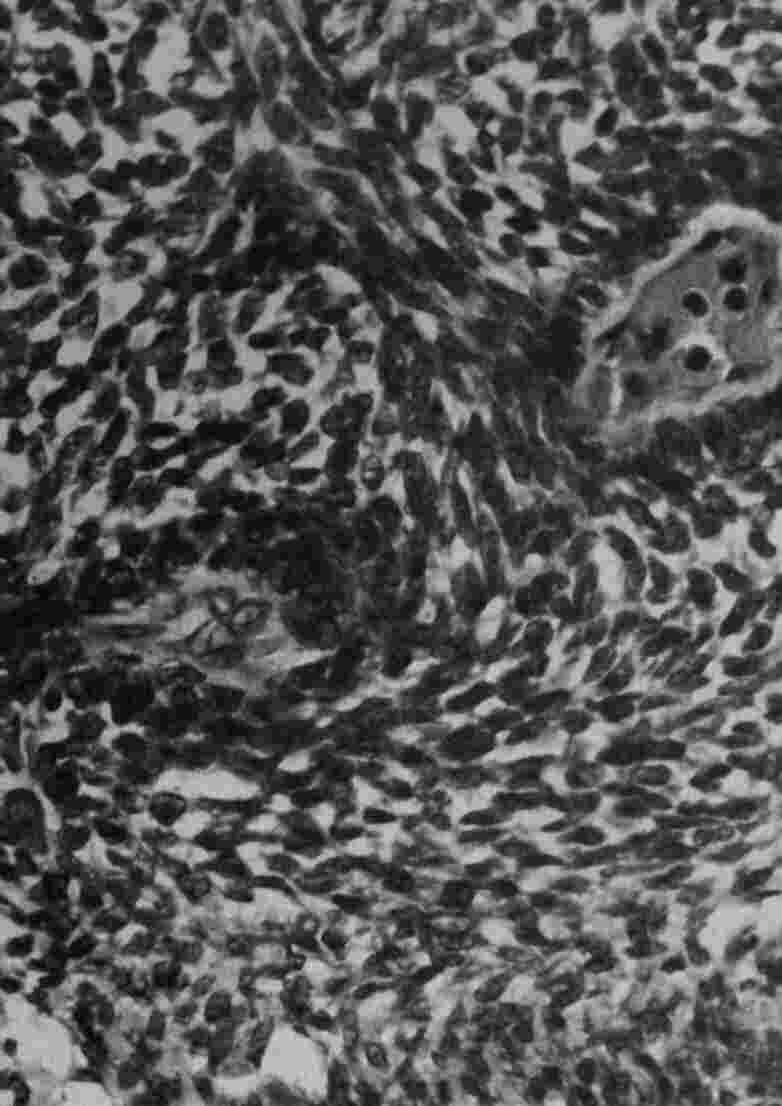 |
Histology shows a combination of spindle cells and epithelial cells, with the palisading effect .